HCC Medicare Advantage Background and Overview
HCC Medicare Advantage Background and Overview
As a follow-up to our previous article “The HCC Coding Specialist: Benefiting payers, providers, and patients” we now delve deeper into the background and overview of HCC risk adjustment for the Medicare Advantage Program.
Background on Payment in the Medicare Advantage Program
The Medicare Advantage (MA) program allows Medicare beneficiaries to receive Part A and Part B benefits from private insurers. Otherwise known as Medicare Advantage Organizations (MAOs) that contract with the Centers for Medicare and Medicaid Services (CMS) to provide benefits as an alternative to the traditional Fee-for-Service (FFS) Medicare program. There has been a steady increase in Medicare Advantage enrollment as a proportion of total Medicare enrollment. In 2003, only approximately 13% of the Medicare population was enrolled in a Medicare Advantage (MA) plan. In 2014, Medicare Advantage (MA) enrollees accounted for 30% of all Medicare beneficiaries. And in 2019, MA enrollees grew to 37% of all Medicare beneficiaries (source: cms.gov).

CMS pays each Medicare Advantage Organization (MAO) a monthly per-person amount for each beneficiary enrolled in its plan. The plan’s bid determines the payment rates. The MAO submits it to CMS on an annual basis. The per-person amount paid to each plan for enrolled beneficiaries adjusts to account for differences in health status between enrolled beneficiaries. This is a “risk adjustment” model, and the Balanced Budget Act of 1997 (BBA) authorizes it. From 1997 to present, there have been several different types of risk adjustment models. But, in 2004, CMS selected a new risk adjustment model to begin using for payment: Centers for Medicare & Medicaid Services (CMS) Hierarchical Condition Categories (CMS-HCC) model, which includes diagnoses recorded on professional, inpatient, and outpatient claims.
CMS-HCC Model overview
 The CMS-HCC model is prospective where data is collected in the base year to determine expected costs for the following year (the “prediction” year). For example, data from 2019 (base year) will predict expenses in 2020 (prediction year). Each segment of the CMS-HCC model relies on data from demographics (i.e. patient’s age and gender) and health status. These are based on ICD-10-CM diagnosis codes to predict costs. To identify the disease diagnoses that predict future healthcare costs, HCC models first organize diseases/conditions into body systems or disease processes, called diagnostic groups (DXGs). The disease processes within each diagnostic group (DXG) fall into condition categories (CCs). Then, delineated into the HCC. ICD-10-CM diagnosis codes rank into categories that represent conditions with similar cost patterns. There are over 9,500 ICD-10-CM codes that map to one or more of the 83 HCC codes included in the 2019 CMS-HCC Risk Adjustment Model (Version 23).
The CMS-HCC model is prospective where data is collected in the base year to determine expected costs for the following year (the “prediction” year). For example, data from 2019 (base year) will predict expenses in 2020 (prediction year). Each segment of the CMS-HCC model relies on data from demographics (i.e. patient’s age and gender) and health status. These are based on ICD-10-CM diagnosis codes to predict costs. To identify the disease diagnoses that predict future healthcare costs, HCC models first organize diseases/conditions into body systems or disease processes, called diagnostic groups (DXGs). The disease processes within each diagnostic group (DXG) fall into condition categories (CCs). Then, delineated into the HCC. ICD-10-CM diagnosis codes rank into categories that represent conditions with similar cost patterns. There are over 9,500 ICD-10-CM codes that map to one or more of the 83 HCC codes included in the 2019 CMS-HCC Risk Adjustment Model (Version 23).
Here’s an example of HCC categorization:
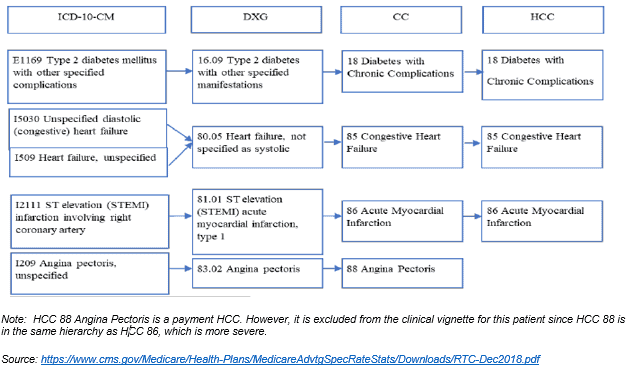
NOTE: HCC 88 Angina Pectoris is a payment HCC. However, it is excluded from the clinical vignette for this patient since HCC 88 is in the same hierarchy as HCC 86, which is more severe (more at: https://www.cms.gov/)
The CMS-HCC model focuses on long-term chronic conditions that impact the probability of future healthcare costs. For instance, diabetes, autoimmune disorders, end stage liver disease, end stage renal disease, chronic obstructive pulmonary disease (COPD), and congestive heart failure (CHF). The CMS-HCC model does not include acute illnesses and injuries that are not reliably predictive of ongoing healthcare costs.
Coding professionals need to review the entire medical record documentation to assign appropriate ICD-10-CM diagnosis codes. Most chronic conditions have an HCC assignment. HCC categories report all conditions that affect the patient’s health status concurrently across the continuum of care. To support an HCC, the medical records must support the presence of the disease/condition. Additionally, they need to include the clinical provider’s assessment and/or plan for the management of the disease/condition. Most organizations use the “M.E.A.T” criteria. Monitoring, Evaluation, Assessment, Treatment for their documentation practices as well as ICD-10-CM diagnosis coding, and HCC assignments.
This article successfully covers how the complexity of documentation, coding, and the patient’s ICD-10-CM diagnosis codes can impact on HCCs. Accurate diagnosis coding is essential for appropriate risk adjustment which drives the most suitable reimbursement for physician services. Be sure that your clinical providers and coders are knowledgeable about HCC documentation and coding! YES HIM Consulting’s team of skilled coding and auditing experts can be your organization’s “go-to” Medicare risk adjustment and coding consultant. Contact YES today. Additional articles will be presented on the YES blog.
