The Importance of Specificity in Documentation and Coding HCCs
The Importance of Specificity in Documentation and Coding HCCs
HCC chronic conditions
As a follow-up to our previous articles on the subject of Risk Adjustment and HCCs, we now review some scenarios of HCC chronic conditions. We also discuss the importance of specificity in documentation and coding. HCC coding is one of YES HIM Consulting’s many specialties; contact our team today for our consulting services or coding support.
Cited in our article “HCC Chronic Conditions and M.E.A.T. Criteria,” HCC risk adjustment is a fundamental method used in health insurance payer programs to account for the overall health and expected medical costs of each individual enrolled in a health plan. Currently, the focus is to effectively address the high prevalence of chronic conditions among Medicare beneficiaries. Active, efficient, and effective management of these chronic conditions is critical; it ensures that Medicare beneficiaries receive the best possible care. It also ensures that the Medicare program is sustainable.
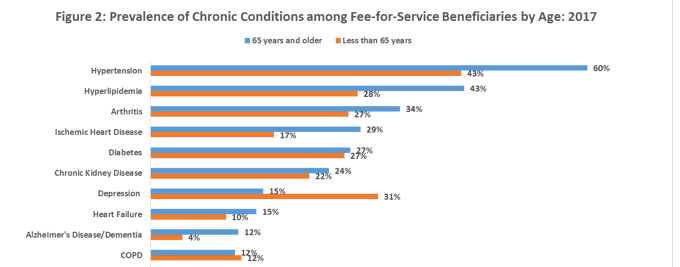
From the most current CMS data (2017), for Medicare beneficiaries 65 years and older, 60% have been diagnosed with hypertension. In addition, 43% have been diagnosed with hyperlipidemia (high cholesterol), 34% with arthritis, 29% with ischemic heart disease and 27% with diabetes.
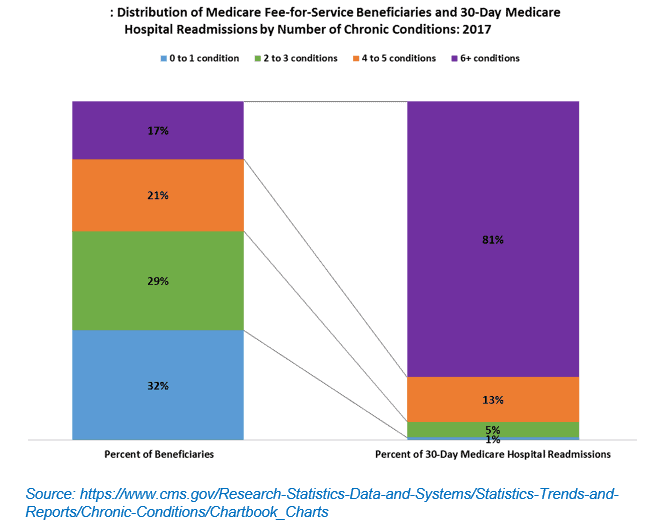
Also, according to the most recent CMS data (2017), over two-thirds of Medicare beneficiaries are living with two or more chronic conditions. This equates to 99% of the overall 30-day Medicare hospital re-admissions.
Accurate and complete documentation of chronic condition diagnoses by clinicians is an essential component of the risk adjustment and the HCC process. Providers are required to document all conditions they evaluated during every face‐to‐face visit. It is also imperative that the documentation of a disease/condition be as specific as possible. Specificity can make a difference in the patient’s treatment plans, as well as accurate code assignments; this then leads to appropriate HCC assignment and payment.
Example one: Capturing complications accurately:
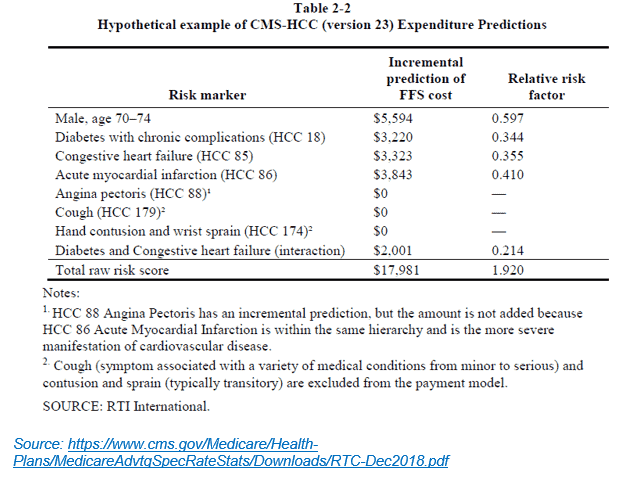

Utilizing the example above, if the documentation only listed diabetes mellitus with no specificity or complications, the HCC changes from HCC 18 (diabetes with chronic complications) to HCC 19 (diabetes without complication). The relative risk factor for HCC 18 is 0.344, but the relative risk factor for HCC 19 is only 0.109. This could result in incorrect data submission. It could also result in a decrease in the total raw risk score from 1.920 to 1.685 and predicted cost (payments) from $17,981 down to approximately $15,784*. This $2,197 reduction in payment is for one patient. With 27% of Medicare beneficiaries reported as having diabetes, there is a high probability that many of these patients have chronic complications of the disease. Not capturing these complications could result in a significant overall loss in payment.
Example two: Accurate documentation and coding specificity
Another example in the importance of accurate documentation and specificity coding would be major depressive disorder. The ICD-10-CM diagnosis code for major depressive disorder is not an HCC. However, if the major depressive disorder is specified in the documentation as mild or moderate, a single episode would result in an HCC 59 assignment; this also includes an additional relative risk factor of 0.355, and an additional predicted cost (payment) of $3,325*.
Example three: Diagnosis specificity
A third example is the specificity of the diagnosis of morbid obesity. Many times, the documentation lists BMI, but there is no record of morbid obesity. Both diagnoses are essential for appropriate code and HCC assignments. For instance, if the document records the patient’s BMI at 40.5, the coder will not assign a code and, therefore, no HCC. However, if the coder also documents the diagnosis of morbid obesity, then the specialist can accurately assign the codes. This results in an HCC 22 (morbid obesity), an additional relative risk factor of 0.369, and an additional predicted cost (payment) of $3,457*.
*Note: In the payment year 2019, the denominator used to create relative factors for all segments of the CMS-HCC model is $9,367.34. CMS calculated this using a 2015 cohort of FFS beneficiaries (2014 diagnoses). Source: https://www.cms.gov/Medicare/Health-Plans/MedicareAdvtgSpecRateStats/Downloads/Advance2019Part1.pdf
It is also important to note that in order to support an HCC, documentation must support the presence of the disease/condition. It also needs to include the clinical provider’s assessment and/or plan for management of the disease/condition. Most organizations use the “M.E.A.T” criteria. (See our previous article for an explanation of the M.E.A.T. criteria). Now is the time to review your providers’ documentation practices and coding specificity. Helping organization’s navigate HCC coding is one of YES HIM Consulting’s many specialties; contact our team today for our consulting services or coding support.
